July 2019
There's nothing like a terminal diagnosis to remind you that you have waaaaay too much stuff. And if you do not do something about it, some of the people you love and adore are going to be lumped with the enormous task of sorting it out. I mentioned in the
previous post that when death seems quite imminent, you can focus on the task of getting rid of stuff. But when a new treatment pushes back your own personal "deadline", the urgency of the task wanes considerably. Currently I do not have any solution to that.

The changes in forecast lifespan have recurred throughout my time with cancer. Sometimes death seems like a speeding road train with its headlights on high beam, tail-gating you. At other times you are aware that the truck is somewhere behind you, but your focus is no longer in the rear view mirror, but on the road ahead.
When I started with
hepatocellular carcinoma (HCC), successful surgery seemed like the end of my immediate thoughts of the threat of death. Then, when metastases were detected a year later, treatment options, survival and end of life care come to the fore. At that time there was only one drug treatment option. After I developed a toxic response to that drug I knew there was nothing else for me. But then, just before Christmas 2017, I was told that there was now one other possibility. A new drug, still undergoing clinical trials. The challenge for my specialist was figuring out how to access this new immunotherapy drug, just beginning to be used for HCC. He was no doubt very busy over the Christmas holiday period, writing up applications to various bodies to obtain access. I was not eligible for the ongoing clinical trial as recruitment had just closed. But he made a case to the drug company for a compassionate access program.
That drug,
nivolumab, was delivered by intravenous infusion. This meant I needed to be in my home town every two weeks for the foreseeable future. Never mind though. I developed no unmanageable side effects and we could learn to plan around the fortnightly trips to the IV Lounge. Life became normal again. Except for one afternoon a fortnight, I virtually forgot I had cancer. Things were sweet for about 15 months. Then a tumor marker on the blood and a CT scan suggested that my good buddy, nivolumab was no longer working for me. For several months it was not clear if I needed to divorce nivolumab and enter into a new marriage with the new kid on the block lenvatinib (Lenvima). This drug worried me. It was a brother drug to sorafenib (Nexavar) which I'd only been able to tolerate for 10 days because of a serious adverse reaction.
You start to analyse and discuss the research studies about your drugs: what trials have been undertaken, are the results available yet, what is the side effect profile, what is the effectiveness (Overall Response Rate, Time to Progression, Progression Free Survival).
You set up a
Google Alert for hepatocellular carcinoma and the drug you are on, so you can keep up with the latest health care news.
You weigh up the pros and cons. What is the probability of the drug working vs the probability of intolerable side effects? Despite these analyses, you have no way of predicting your individual responses to the drug. Which group will you fall into - the group which did gain a benefit from the drug or the group that didn't? The group which experienced bad side effects, or the group that didn't?
I was lucky to be offered lenvatinib which had been placed on the Australian Phamaceutical Benefits Schedules only days before. Instead of paying AUD9,600 a month for daily capsules, the Australian Government subsidy meant I would pay just AUD6.50.

So life with cancer is a series of new decision points, decisions that must be made with imperfect information. It is a special kind of emotional roller coaster, with some smooth bits in the middle.
My partner and I approached each consultation with the specialist with a list of questions and discussion points we'd prepared. We realised beforehand that there would probably be no clear answer to some of the questions, but we still had to ask.
We took copious notes and discussed them afterwards. Invariably one of us would have picked up points the other had missed. There's such a benefit from having two pairs of ears.
In the end you just have to decide what seems right at the time.
Whether you see an oncologist or a hepatologist depends on who you can develop a good rapport with, more than anything. I used to think that oncologists want to push you towards the most aggressive treatment regimes and would not support your decision to stop pointless treatment. But perhaps not all are like that. I would like to see the cancer under control of course, but not at any cost. The quality of my life is far more important than the quantity.
I was also very fortunate that the public hospital HCC clinic I attended provided access to a specialist nurse by phone and email. If a new side effect appeared, the nurse was interested and responsive, suggesting ways of managing it and arranging a prescription, if needed. She checked on me weekly and also helped coordinate between the hepatologist and my general practitioner (primary care physician) and any other specialists involved in my care. Best of all she encouraged me to get out there and enjoy a normal life.
This nurse liaison service is quite wonderful. It's a service not so evident for all those attending a private clinic, despite the large difference in out of pocket costs. Cancer care seems to be more disjointed in the private sector than the public sector, based on my own experience and that of friends and acquaintances. Things happen to patients between consultations. People living with cancer need a way of being supported in a more continuous manner by people who understand and are trained in this field.
Post script written four months after the above (Nov 2019)
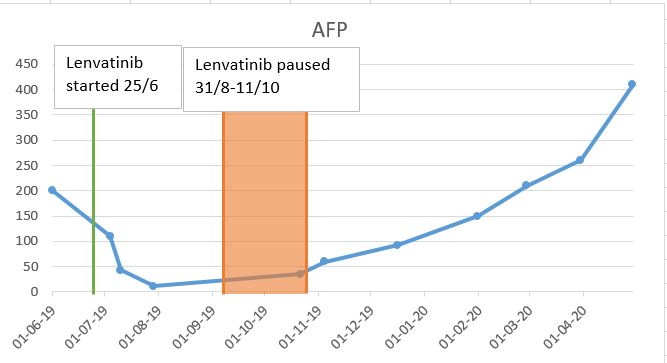
In late June I'd decided to have a go with the new kid on the block, lenvatinib and this was going well. The tumor marker was coming down, no new tumors, perhaps slight decrease in size of some of the existing ones. I felt well.

Then I didn't feel well. Backache, chronic cough, weight loss, fatigue and breathlessness, increasing throughout August 2019. Then a CT scan revealed "
ground glass" - white opaque areas in my lungs. Either I had pneumonia or
pneumonitis, an immune related inflammation of the lungs. Another hospital stay, this time for 3 weeks. Firstly they had to determine which was the cause, pneumonia or pneumonitis. The treatment for pneumonitis, steroids, could have a disastrous effect if it were an infection. I spent 10 days getting pumped with antibiotics and tested for every kind of lung infection, all the while getting sicker and sicker, in respiratory failure on 15 litres of oxygen a minute, bed bound. Finally a specialist decided it was time to start steroids!


And I slowly began to improve, get my appetite back, sit out of bed, take a few tentative steps. I had pneumonitis, believed caused by a delayed reaction to the previous drug, the immunotherapy drug nivolumab, which can over-activate the immune system so that it attacks your healthy body.
Seven weeks later, after lots of support from family, friends, health professionals, a regular home rehab program of exercises and walking, I no longer need the oxygen around the house, just when exercising and walking longer distances. I am getting better.
I'd had to stop the cancer drug lenvatinib when I was in hospital as I was so ill. Have now resumed it and am back on track.